 The NASW Social Work Code of Ethics is a very helpful but demanding document. It asks us to live a cognizant life both at work and at home. If we take this document seriously, and we certainly must, it demands that we are prepared to confront things not in concert with the Code.
The NASW Social Work Code of Ethics is a very helpful but demanding document. It asks us to live a cognizant life both at work and at home. If we take this document seriously, and we certainly must, it demands that we are prepared to confront things not in concert with the Code.
Unfortunately there is a massive failure by the entire social work industry to adhere to that code going on right now.
If you will, think about a southern, rural town in the early 1950’s. Imagine you are there to give a workshop to the townspeople on racism. Can you guess their reaction to your words about racial equality? Their daily habits and way of life is based on something far from what you are describing to them. What do you think they would say and do? My guess is they might politely listen but after leaving conclude that you were some sort of nut — a “n***** lover” or even more likely an interloper who hates them and their way of life.
In some ways I feel like that person right now. There is a form of discrimination that is clearly present, potently hurtful and yet most of those around me are hostile to hearing about it. They just don’t and won’t see it. If you call attention to it, if you point to the elephant in the room, they become hostile.
Who is the group that faces discrimination that no one sees? It is men and boys. And the treatment of them in the arena of social work has taken a very, very disturbing detour from the NASW Code of Ethics for quite some time now.
Where it concerns the interrelationship between men and women our early survival mandated cooperative gender roles. Men would provide, protect and risk in order to ensure the safety of women and children. Women provided the essential immediate care of children.
This arrangement is what we have come to know as gynocentric in that the roles taken on by men and women hinged on fact that women and children had to be protected at all costs. While both roles are or were vital in the overall picture, life and limb sacrifices, the role of protector and provider fell on the shoulders of the male. In short, the male is replaceable. The women are not, because men can’t have children.
This arrangement worked spectacularly for a long time. However, human advancement, through the cooperative efforts of men and women, resulted in a world where gender roles are generally not essential for human survival. We have far fewer concerns over our immediate safety than we did on the African Savanna and technology has made many professions accessible to both men and women. Accordingly, women’s roles have evolved and expanded, affording them the opportunity to make more conscious choices, and to experience more freedom than strict gender roles could have ever afforded.
Men, however, have lagged behind in this area and that is where we start to encounter some of the problems that they face today. To more fully understand this, we must take a look at cultural development through the gynocentric lens.
Even before the industrial revolution, while the male role was functional and successful without question, it was one of significant, unrecognized and unseen sacrifice. Of course that made sense. Were humans to practice the same protection and compassion for men as they did for women, it would have destroyed us. In an environment of hardship we could not afford to busy ourselves with men’s suffering and pain. That unrecognized burden was what kept us alive.
Men’s roles threw them into positions where people just didn’t know if they would ever return home at any point. Whether in the Paleolithic realm of hunting and tribal conflict, or more modern warfare, the certainty of any man’s survival was never assured. When there is constant uncertainty about a person’s fate we tend to detach for our own psychological benefit. We see them as more disposable and basically live in a state of preparedness for their possible demise.
Let’s take an example. Those who are designated to die in war are treated like heroes if they accomplish the miraculous and survive. That “heroism” is offered to young men as a standard of manhood in order to have them fulfill the expectation of sacrifice when needed. When something or someone is seen as disposable we generally ignore their pain and hardship. Indeed, most antiwar sentiment in America is based on the fact that we are killing, not because we are dying. That is expected of the disposable sex.
In the 1980’s and 1990’s, when I worked as a psychotherapist with many traumatized men and women, it was clear that society’s focus was to help women suffering from emotional trauma. Matters became a lot more fuzzy where it concerned men’s pain. I found out very quickly that a man’s emotional pain was taboo. No one wants to hear it, people want to run away.
Honestly and compassionately addressing men’s pain usually triggers an instinctive fear that in doing so those men will no longer be available to provide and protect. They become, at least in our unconscious minds, a liability that we cannot afford.
It took me some time to understand that this fear created an empathy gap that is still rampant in the field. Even in what is supposed to be an enlightened field of work, we are operating on some level as though compassion for men will bring us to ruin. This detachment, indifference to and even hostility toward men’s pain and hardship will be made quite visible to you in the remainder of this article.
You will also see how and why social work currently operates as a professional culture in violation of the NASW Code.
We will demonstrate these issues one by one by first quoting from the code and then documenting how it is systematically violated. Let’s start with discrimination by laws.
Here’s what the code says:
- 4. SOCIAL WORKERS’ ETHICAL RESPONSIBILITIES AS PROFESSIONALS 4.02 Discrimination Social workers should not practice, condone, facilitate, or collaborate with any form of discrimination on the basis of race, ethnicity, national origin, color, sex, sexual orientation, gender identity or expression, age, marital status, political belief, religion, immigration status, or mental or physical disability.
That is very unambiguous language. It paints a clear, ethical path that social workers must follow when performing professional duties. Failing to follow those edicts is not just an ethical violation, it is an act of moral turpitude and an abuse of individuals entrusted to their care.
Let’s take a look at an example.
Domestic Violence
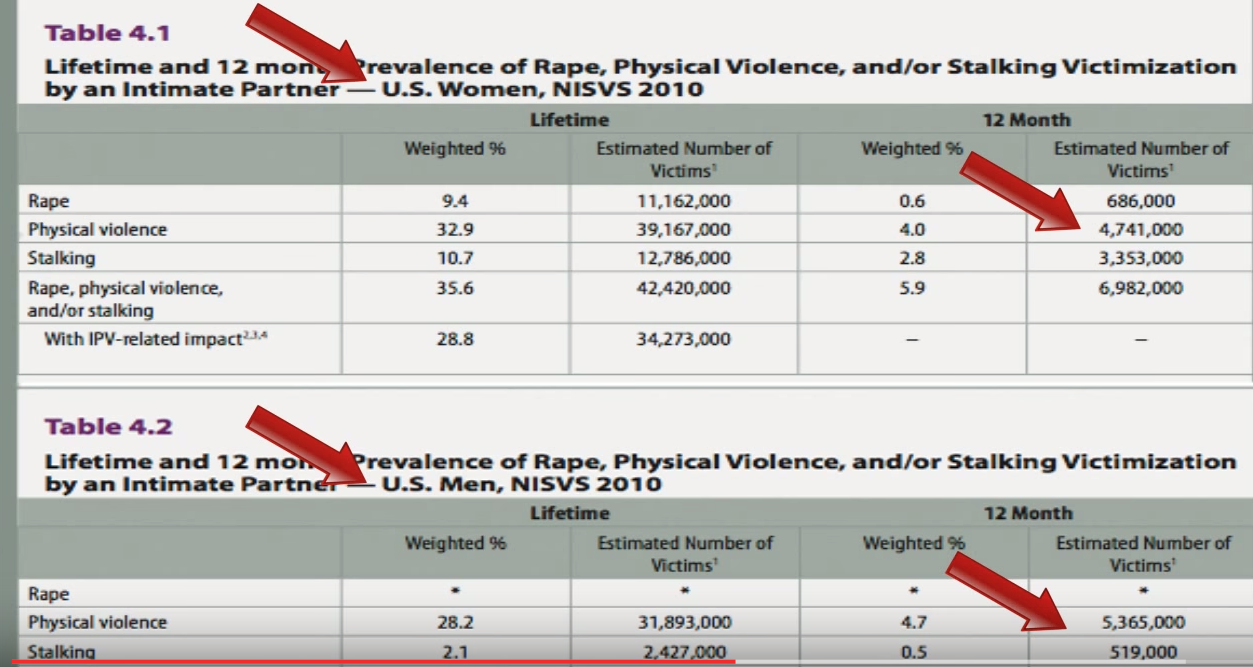
We know now that men are a significant portion of the victims of domestic violence. The latest CDC research confirms this and in fact states that in the past 12 months men were 53% of the victims of domestic violence. However, the services for domestic violence are astoundingly built to serve only women. This is overt discrimination.
We know from the research of Denise Hines1 that when men seek help as victims of domestic violence at these female only services for victims they are not only turned away, they are often told they are the abusers. Many battered men have reached out for help for themselves and their children only to be offered anger management classes because that is all these facilities will offer men.
This is profoundly destructive. It is, if we are to be honest, a second perpetration of abuse, this time at the hands of professionals who are ethically bound to do just the opposite of what they are doing.
Nearly everything related to the amelioration of domestic violence has been built for women. Social workers have said very little about this but the courts have started to acknowledge the discrimination that men face as victims of domestic violence.
In the Woods et. al. vs California2 case in 2008, a Superior Court in Sacramento, ruled that male domestic violence victims had been unconstitutionally denied services. The court held that state laws violated men’s equal protection rights by excluding male victims from state-funded domestic violence services. The court found: “domestic violence is a serious problem for both women and men” and that “men experience significant levels of domestic violence as victims.”
Then, in October 2009, a West Virginia judge3 struck down state rules for regulating domestic violence shelters because they operate “on the premise that only men can be batterers and only women can be victims” and “exclude adult and adolescent males from their statutory right to safety and security free from domestic violence based only on their gender.”

It’s clear that this problem is now widespread in the United States. Yet where is any objection to any of this being raised by social workers, who are deeply embedded in the provision of services to the victims of domestic violence?
Consider this. In California and West Virginia they were sued and found culpable for violating anti-discrimination laws. In both states they were found guilty of violating laws that almost exactly replicated their code of ethics.
So where are the professional sanctions against them? What NASW sanctions were placed on the people responsible? What investigations were done? Why, despite the fact that there is open and systemic discrimination against men practiced by social workers, is the NASW not cleaning house?
It is because the NASW draws the line at adhering to their own ethics where it concerns men. Where it concerns men, it is the people responsible for enforcing those ethics who are committing the most egregious violations of the same.
Family violence against men is seen as humorous.
In fairness it must be said that social workers are also people. And people, generally speaking, are detached from men’s pain.
Their humanness, however, does not excuse them for doing damage instead of rendering aid. They are educated people who must be expected to operate in accordance with their own professional codes. Just as they are expected to rise above every other area of potential bias they may have toward other groups, they are also beholden to practice the same with men and boys.
If you are a social worker working in the area of domestic violence are you aware of this discrimination? Are you speaking out against it? Remember, being aware and doing nothing is what the code calls “condoning and facilitating.” As social workers we need to stand up for those who are facing discrimination and in this case it is men and boys. If you do see this and say nothing you are a part of the problem. You are living in a small, rural town in the 1950s.
Will you follow the code and stand up for these men who face discrimination?
OB/GYN
Social Workers in hospitals pediatric or OB/GYN units should be aware that there is severe discrimination going on right under their noses, a discrimination that is built right into our laws. Baby girls are protected from having their genitals mutilated by law. No exceptions for cultural or religious differences. No exceptions for anything, as it should be. Penalties for breaking this law are severe. At the same time genital mutilation of baby boys is one of the most popular surgical procedures in America. This is not a minor prick of the skin.
And there is now an abundance of medical research concluding for the most part that circumcision is actually just a euphemism for genital mutilation. There are deaths associated with this medically unnecessary procedure and now a variety of confirmed and suspected negative side effects.
Circumcision on average removes 6,000-10,000 nerve endings of erogenous tissue, nearly as many nerve endings as the entire female clitoris which many estimate to have around 8,000 nerve endings. The adult male equivalent in terms of amount of skin removed is the size of an index card, about 3 x 5 inches.
From the group, Doctors Opposed to Circumcision:
Memory starts before birth and newborn infants have fully functioning pain pathways. One would expect, therefore, to find psychological effects associated with the painful genital cutting operation.
Post-traumatic stress disorder (PTSD) is a normal response to an abnormal event. Neonatal genital cutting is an event in which a newborn infant experiences extreme levels of pain, terror, and helplessness, so it fulfills the criteria as a psychogenic for PTSD. Levy (1945) reported that children experience behavior problems, such as night terrors and a fear of nurses and doctors, after surgery, including circumcision. Cansever (1965) tested boys before and after circumcision and reported that the ego seeks safety in total withdrawal. Levy found their symptoms to be similar to combat neurosis, now known as PTSD. Taddio et al. (1997) studied the behavior of babies at first vaccination.
They found that circumcised boys have a much stronger reaction to pain of vaccination than do girls and intact non-circumcised boys, which the authors suggested is an “infant analogue” of PTSD. Other authors also have reported PTSD in circumcised males. Rhinehart (1999) reported four cases of PTSD secondary to neonatal circumcision in middle-aged men that he encountered in his psychiatric practice. Ramos & Boyle (2001) reported PTSD in 70 percent of Filipino boys who experienced ritual circumcision and 51 percent of Filipino boys who experienced medical circumcision.

Circumcised males often feel great anxiety regarding their circumcision. This manifests itself in a reluctance to talk about circumcision or an assertion that “I’m circumcised and I’m fine.” van der Kolk (1989) reports some traumatized males also have a compulsion to reenact or repeat the trauma. These feelings emerge as the “adamant father” syndrome. Typically, a circumcised father will irrationally and adamantly insist that a son undergo circumcision, although this is contrary to contemporary medical advice.
Some circumcised doctors also exhibit anxiety by pushing medically unnecessary circumcision on their patients or writing medical journal articles to defend the practice. Such articles are “flawed papers that dismiss the harm and exaggerate alleged benefits.” This has caused the medical literature on the subject of male circumcision to become voluminous and polarized because other doctors write letters and articles to refute the false claims of circumcised doctors.
Circumcision of the newborn usually is performed in the first week of life (the perinatal period), and, as reported above, clearly is traumatic for most boys. Several authors report that perinatal trauma causes self-destructive behavior in adult life.
Circumcision is cyclic trauma. Many males, who were circumcised as infants, grow up to become circumcisers themselves, in an unending repetitive pattern of abuse.
You can read the entire document here with sources.
http://www.doctorsopposingcircumcision.org/DOC/statement06.html
What we find, when considering all the evidence about circumcision is that the only difference between male and female genital mutilation is that one is socially acceptable and one is not. It seems obvious when you consider the longstanding, programmed indifference to the pain of males, which is which and why.
Here are some more sources demonstrating the severely negative impact of circumcision on infants, their parents and how those consequences follow the victims through life.
http://www.cirp.org/library/psych/goldman1/
https://www.psychologytoday.com/blog/moral-landscapes/201501/circumcision-s-psychological-damage
http://www.circinfo.org/Warren.html
There is an abundance of other research. True enough, there are studies that conclude that circumcision does not produce significant problems for men but as we find in criticisms of those studies, circumcised researchers and circumcised doctors who perform circumcisions both have emotional and financial investment in the procedure.
What is most damning in my mind though is that social workers in the OB-GYN and neonatal fields do not generally deliver any information to parents that might make them reconsider whether circumcision was healthy for their child.
This failure to educate and inform their clients, or indeed to inform themselves of the research is a clear violation of NASW ethical codes.
Part of what drives this is that male genital mutilation is a profitable venture. Aside from the money made doing the procedure the foreskins can be sold for around $400 each depending on how they are used.
Some are used for research while some are turned into very expensive women’s facial cream advertised on Oprah. We are now aware that these circumcisions, the majority of which are conducted without anesthesia, are causing psychological problems and physical problems for the boys and men who are unfortunate enough to have been subjected to them.
Alexithymia (a deficit in emotional acumen and experience) and PTSD have both been connected to male infant circumcision and it is doubtless that many more negatives will be found. In fact much of what we know about girls who have faced genital mutilation is also being found true for the millions of little boys and the men they become.
Social workers are rightly very concerned about female genital mutilation but are failing roundly to address this concern on behalf of boys. If you are a social worker are you following the code and speaking out against the mutilation of children for profit, or are you turning a blind eye to the matter altogether as long as the victims are boys?
And have you considered that if you are working with a family going through childbirth and postnatal care, and you have remained silent about this issue that you can reasonably considered accessory to the abuse?
These are tough questions but as social workers we are not ethically afforded the luxury of failing to answer.
Now let’s move to an area where men and boys face discrimination not from laws but from societal ignorance and lack of compassion.
Here’s what the code says:
6.04 Social and Political Action (a) Social workers should engage in social and political action that seeks to ensure that all people have equal access to the resources, employment, services, and opportunities they require to meet their basic human needs and to develop fully.
Places men face discrimination based on ignorance and/or lack of compassion.
Suicide
Did you know that eight out of ten completed suicides are males4? Have you heard that stat tossed around? Have you ever heard a social worker rise up to say that we are ignoring the glaring problem of male suicide? Probably not. The gynocentrism in modern social work does not permit for men, as a group, to have any of their issues given due prominence. This is true even when men are killing themselves at four to five times the rate of women.
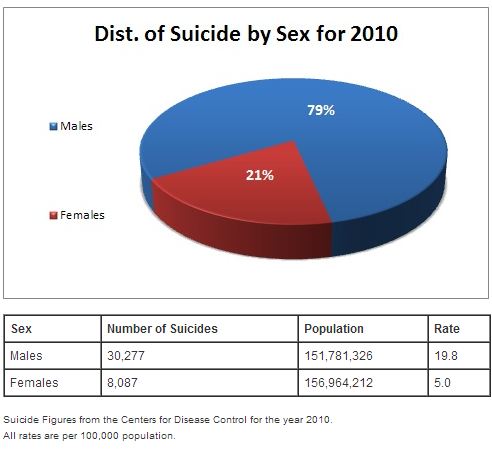
NASW studied suicide some years ago. The study focused on girls and suicide. I asked at the time why they didn’t study boys since boys were 80% of the victims and they said the funding requested the study focus on girls. Sadly, this is not uncommon. The focus of the media, researchers and clinicians is on girls and women even though they are a fraction of the victims. As a Social Worker, do you see this discrimination? Shouldn’t a commensurate amount of research be done based on those who are most victimized? Shouldn’t any conference on suicide have most presentations related to male suicide and what to do about it? Shouldn’t we create services designed for those who are most at risk? We need to stand up for the victims and potential victims of suicide that are being ignored and marginalized. Will you stand up for boys and men? Do you think that ignoring that question puts you in direct violation of your professional responsibilities?
Paternity Leave
We all know about maternity leave for women. It is pretty much a standard. But why wouldn’t paternity leave also be a standard? Why is paid leave only given to the mother and not the father? And why are so many social workers so vocal on the need for men to assume more childcare duties yet remain mute about the very kind of legislation that would allow that to happen?
People are starting to wake up to this discrimination. California, Washington and New Jersey have all passed laws offering “family leave” for all, not just for mothers. What does it say about the social work field that they are not pushing similar initiatives in the other 47 states?
Longevity
Men tend to live shorter and sicker lives than women. The fact is that white women have the greatest longevity followed by black females, followed by white males, followed by black males. Both black and white men live shorter lives than both black and white females. Some are thinking that black males are at the bottom since they face the burden of both racism and of being male.
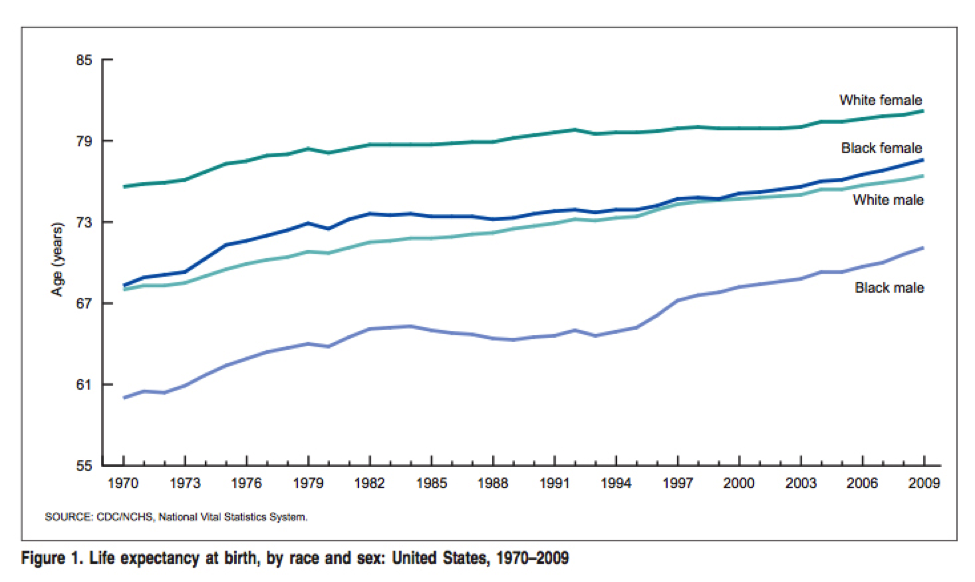
“‘Being male is now the single largest demographic factor for early death,” says Randolph Nesse of the University of Michigan in Ann Arbor. “If you could make male mortality rates the same as female rates, you would do more good than curing cancer.”
Nesse’s colleague Daniel Kruger estimates that “over 375,000 lives would be saved in a single year in the US if men’s risk of dying was as low as women’s.” (New Scientist Magazine, July 2002)
Men die earlier and more often than women from nearly every major cause of death except for one, Alzheimer’s. And the reason for that is that they do not live long enough to compete for that honor.
Even with the longevity and poor health experienced by men what we find is that the services available to them are considerably less than what is provided for women. The United States has seven national offices for women’s health but none for men. They have web pages for womenshealth.gov and girlshealth.gov but none for menshealth.gov or boyshealth.gov. Why do we discriminate and treat men and women so differently? As a Social Worker are you speaking out and standing up for the men and boys who are obviously being marginalized? If not, are you violating our code of ethics?
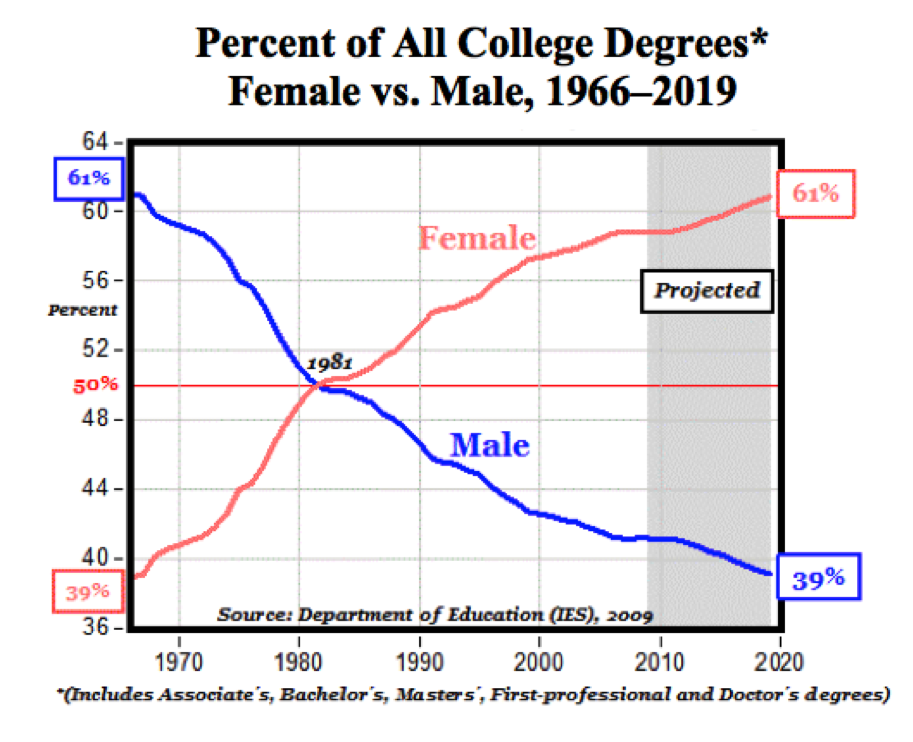
Education
The roles in education have been reversed. What was once considered discrimination against women and girls in their 22% deficit in college degrees has now reversed. It is the boys and men who are getting far fewer degrees than the women and girls. The difference? Now we don’t call it discrimination against boys — we call it empowerment of girls. The disadvantage and discrimination of the boys and men is simply ignored and reframed as a positive. As a social worker are you willing to stand up against this discrimination against boys and men?
I hope you are starting to see the profound bias facing men and boys in today’s world, and in the way that that the social work field is not just ignoring, but facilitating that problem.
The hardship and discrimination they face is ignored and worse, they are villainized and blamed for the problems they experience. Where did Social Workers learn this? In grad school. Our social work education is clearly anti-male and is in dire need of an overhaul to close the empathy gap, and to restore the social work profession to its own ethical standards. If we are educating and training social workers to violate their own code of ethics then it stands to reason that we are left with a pervasive problem throughout the field. We are left with the disturbing reality that the field is the problem.
Part Two will focus on Social Work Education and its anti-male bias.
References
- Douglas, Emily M.; Hines, Denise A.; McCarthy, Sean C.Violence and Victims, Volume 27, Number 6, 2012, pp.871-894(24)
Abstract:
Research since the 1970s has documented that men, in addition to women, sustain intimate partner violence (IPV), although much of that research has been overlooked. A growing body of research is examining the experiences of men who sustain female-to-male IPV, but there is still much to be learned. This exploratory study assesses the experiences of 302 men who have sustained IPV from their female partners and sought help from 1 of 6 resources: domestic violence agencies, hotlines, Internet, mental health professionals, medical providers, or the police. We examine what demographic characteristics and life experiences are associated with where men seek help and how they rate those experiences. We make recommendations for agencies, service providers, and first responders about how to tailor services for this specific population and their families.
excerpt – “This is just basic unfairness. It’s raw gender bias,” said Harvey D. Peyton, attorney for Men & Women Against Discrimination.
The West Virginia legal challenge is among a growing number of battles being waged across the country by groups that allege state laws requiring gender-neutral programs are skewed by discriminatory rules and regulations that embrace gender biases.
Resources
- These three reports were written by the Maryland Commission for Men’s Health and explore the problems of domestic violence, suicide, and men’s health.
- Youtube’s with more information on Domestic Violence, men’s issues,
Tom Golden is the author or three books, Swallowed by a Snake: The Gift of the Masculine Side of Healing, The Way Men Heal, and Helping Mothers be Closer to Their Sons: UnderStanding the Unique World of Boys. Tom was the creator of the youtube channel Men Are Good , was in the Red Pill Movie, and served as the vice chairman of the Maryland Commission for Men’s Health. He has been a therapist in private practice for over 30 years.